Robotic Partial Nephrectomy: Kidney-Sparing Surgery for Renal Tumors- Dr. Zaheen Khan, Urologist and Robotic Surgeon
Robotic partial nephrectomy (RPN), also called robot-assisted partial nephrectomy (RAPN), has rapidly become a preferred kidney-sparing operation for many patients with localized kidney tumors. Performed using a surgical robot, the operation removes only the tumor and a small rim of healthy tissue rather than the entire kidney. This article explains what RAPN is, why it is chosen, who is a candidate, what the operation involves, risks and outcomes- Dr. Zaheen Khan, Urologist & Robotic Surgeon.
What is Robotic Partial Nephrectomy?
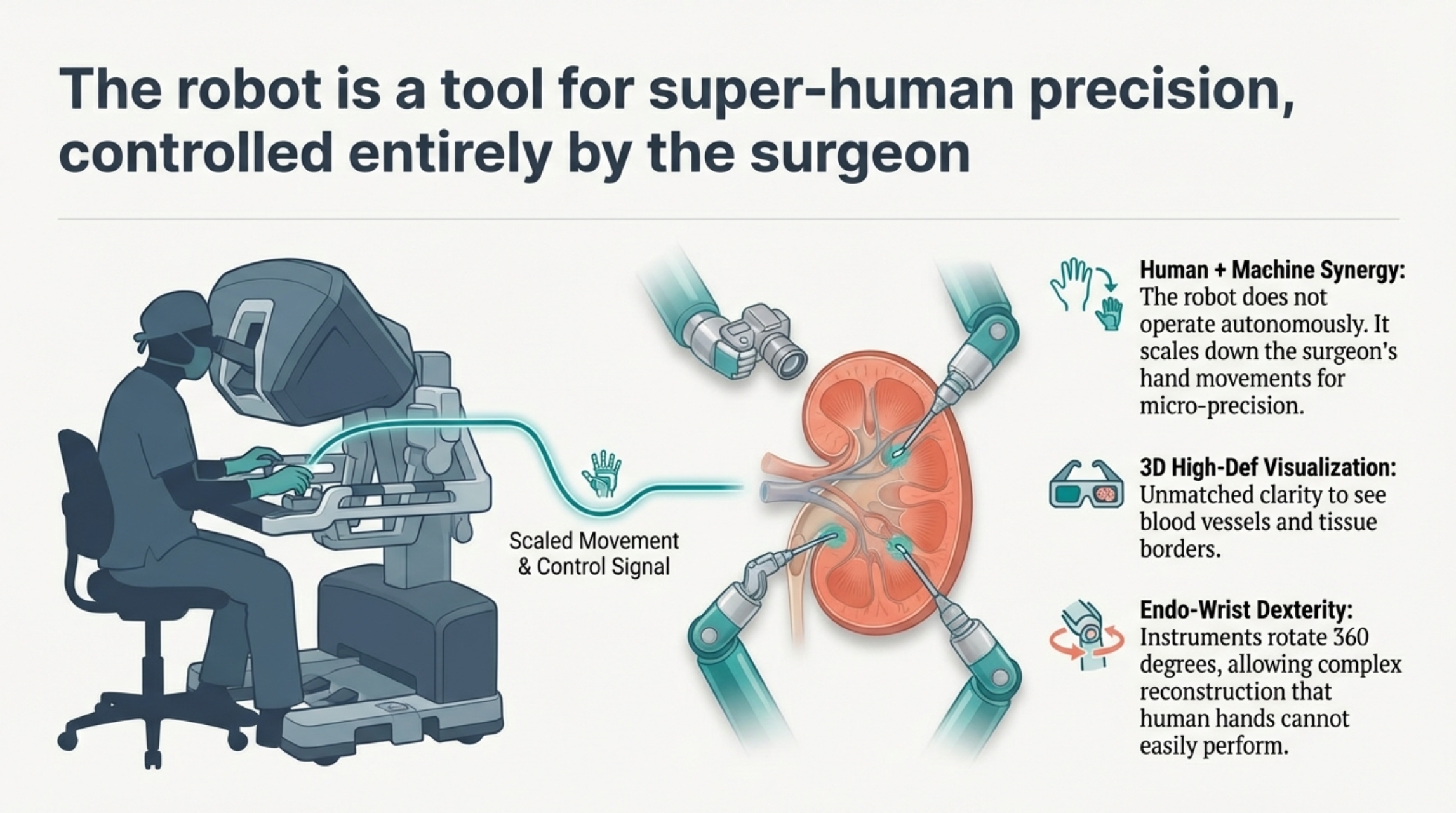
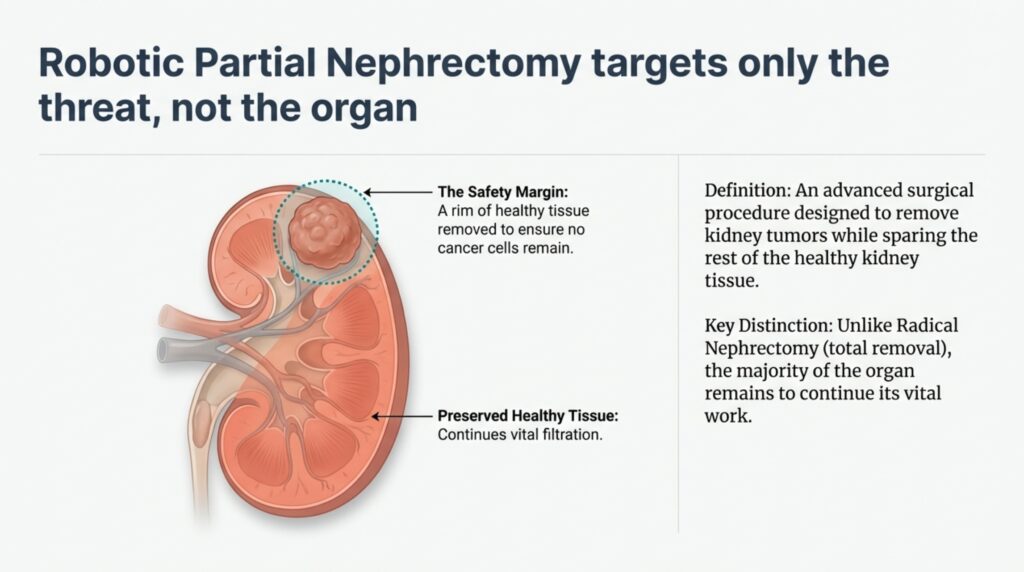
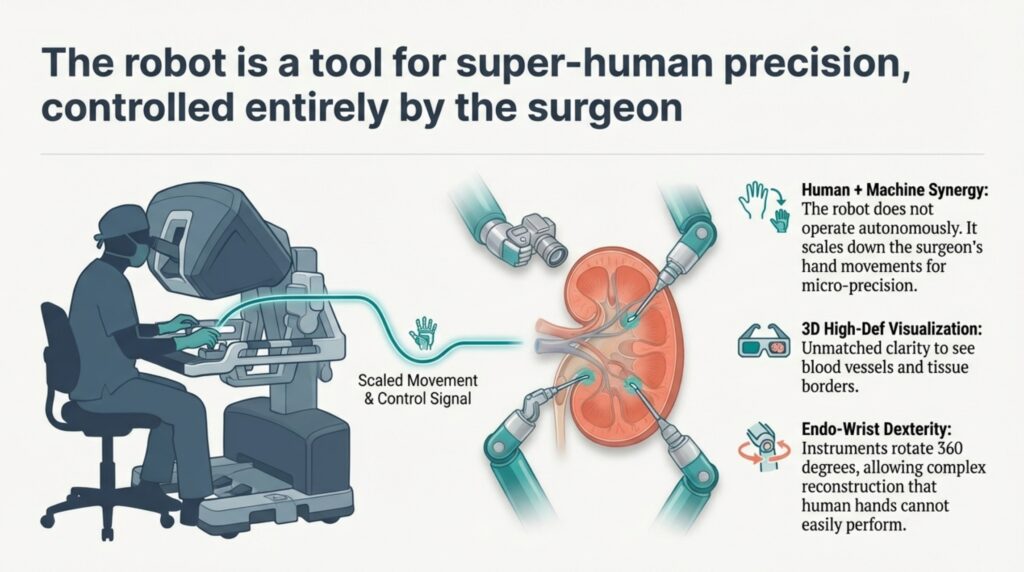
Robotic partial nephrectomy is a minimally invasive surgical technique that allows precise removal of a renal tumor while preserving as much normal kidney tissue as possible. The robotic platform provides the surgeon with a three-dimensional magnified view, highly articulated instruments that mimic wrist movements, and tremor filtration — all translating into fine dissection and meticulous suturing. The main goal is nephron-sparing surgery: treat cancer effectively while preserving renal function.
Why preserve the kidney? The rationale for partial nephrectomy
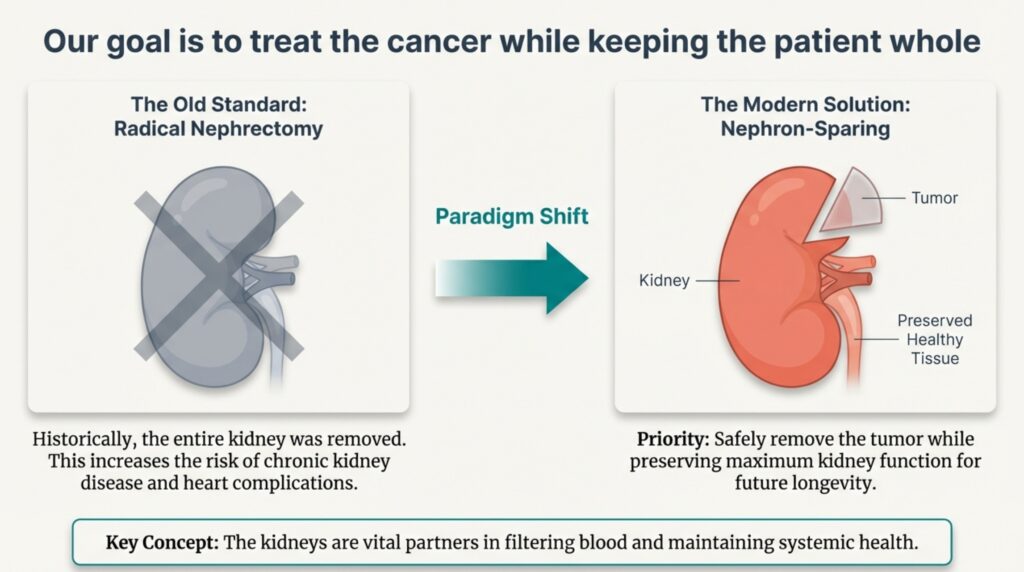
Evidence and international guidelines emphasize preserving renal tissue when oncologically safe. Removing only the tumor (partial nephrectomy) is associated with:
Better long-term kidney function compared with complete removal (radical nephrectomy).
Lower long-term risk of chronic kidney disease and associated cardiovascular events.
Equivalent cancer control for appropriately selected small renal masses.
A variety of research studies and guideline statements recommend nephron-sparing surgery when technically feasible for small (and many moderate) renal tumors. Over time, minimally invasive approaches including laparoscopic and robotic partial nephrectomy have become standard options in many centres.
Advantages of the robotic approach
Robotic partial nephrectomy offers technical and patient-centered advantages compared with open or laparoscopic alternatives in many settings:
Enhanced precision and dexterity: the robot’s articulating instruments and high-definition 3D optics allow precise tumor excision and renal reconstruction.
Shorter warm ischemia time: many series report reduced time of renal ischemia (period during which blood supply is clamped) — an important factor for preserving renal function.
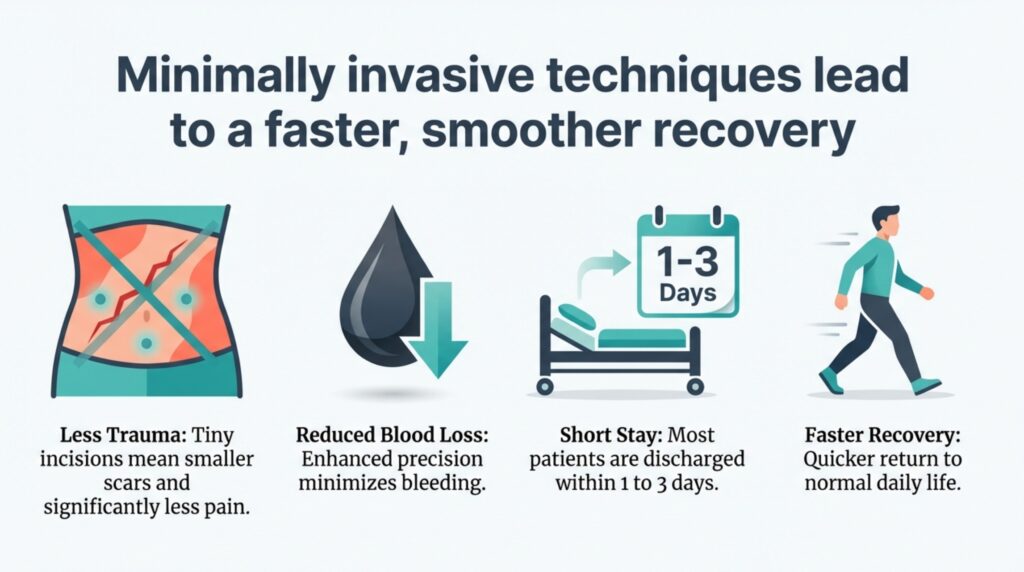
Less blood loss and quicker recovery: robotic approaches frequently report lower intraoperative blood loss, shorter hospital stays, and faster return to routine activities.
Ability to manage complex tumors: as surgical experience grows, many complex and centrally located tumors that once required open surgery are now resected robotically.
Shorter learning curve than pure laparoscopic PN: some comparative research suggests that surgeons achieve proficiency faster with robotic assistance.
It is important to stress that advantages depend on surgical experience, institutional support, and appropriate patient selection.
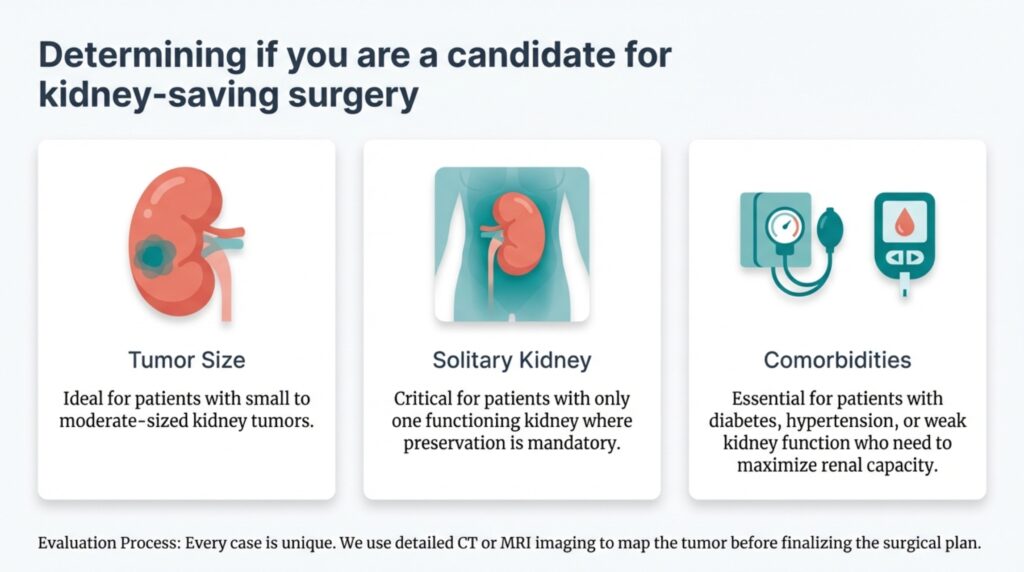
Who is a candidate for robotic partial nephrectomy?
Typical candidates include:
Patients with localized renal masses (commonly stage T1a ≤4 cm, and many T1b 4–7 cm tumors), where oncologic control can be achieved with partial nephrectomy.
Patients with a solitary functioning kidney, bilateral tumors, or pre-existing reduced kidney function — scenarios where preserving renal tissue is particularly important.
Selected patients with more complex tumors may also be candidates at high-volume centres with experienced robotic teams.
Final candidacy is determined after thorough imaging (contrast-enhanced CT or MRI), assessment of tumor location (endophytic vs exophytic, hilar involvement), patient comorbidities, and multidisciplinary discussion.
Preoperative planning and imaging
Accurate preoperative imaging is essential. A contrast CT (CT KUB with arterial and venous phases) or MRI provides details about tumor size, location, relation to the collecting system and blood vessels. Many modern teams use three-dimensional reconstructions or virtual models to plan port placement, identify arterial branches supplying the tumor, and strategize resection planes. Preoperative optimization includes kidney function tests, blood tests, and counseling about possible outcomes and complications.
Technique overview — what happens in the operating room?
A typical robotic partial nephrectomy workflow includes:
General anesthesia and patient positioning. The patient is positioned to provide optimal access to the kidney either via the transperitoneal or retroperitoneal route.
Port placement and robot docking. A few small incisions (ports) are made; the robot is docked.
Tumor exposure and vascular control. The kidney is exposed, the tumor localized, and arterial control is prepared. Selective arterial clamping or main artery clamping may be used depending on anatomy. Techniques that minimize ischemia — early unclamping or selective segmental clamping — are commonly employed.
Tumor excision with margin. The tumor is removed with a small rim of healthy tissue, maintaining oncologic principles.
Renorrhaphy (kidney repair). Careful closure of the defect and any collecting system openings is performed to control bleeding and prevent urine leak.
Specimen retrieval and closure. The specimen is removed through a small incision; hemostasis and drains as needed; ports closed.
Hospital stay is commonly short — often one to three days — and recovery time is significantly quicker than open surgery.
Key outcome measures — the “trifecta”
Surgeons commonly use a composite outcome (often called trifecta) to describe successful partial nephrectomy:
Negative surgical margin (complete tumor removal without residual cancer at the edge).
Minimal ischemia (short warm ischemia time or techniques that preserve kidney perfusion).
No major complications (Clavien-Dindo grade III or higher).
High-volume centers and experienced robotic surgeons report favorable trifecta rates; achieving the trifecta is associated with excellent oncologic and functional outcomes.
Risks and complications
All surgeries carry risk. For RAPN, potential complications include:
Bleeding and need for transfusion (uncommon in experienced hands).
Urine leak if the collecting system is opened (managed conservatively or with intervention).
Injury to adjacent organs (rare).
Postoperative infection or wound problems.
Loss of renal function if ischemia is prolonged or if pre-existing renal disease is severe.
Careful surgical technique, selective arterial control, and immediate access to interventional radiology or blood bank reduce the risk of significant adverse events.
Oncologic safety — is cancer control comparable?
Multiple series and comparative studies show that, for appropriately selected tumors, partial nephrectomy (open, laparoscopic, or robotic) provides similar short- and medium-term oncologic control to radical nephrectomy, with the benefit of superior renal function preservation. For small renal masses, nephron-sparing surgery is the guideline-recommended approach when feasible.
Functional outcomes — preserving kidney health
One of the strongest arguments for partial nephrectomy is long-term kidney preservation. Chronic kidney disease (CKD) has major public health implications because reduced kidney function increases cardiovascular risk. By sparing nephrons, RAPN helps maintain renal function and reduces the risk of dialysis or CKD-related complications later in life.
The role of surgeon experience and institutional support
Outcomes in robotic kidney surgery correlate strongly with the surgeon’s experience and the institutional volume. Facilities with trained robotic teams, experienced anesthesiologists, interventional radiology support, and appropriate perioperative care systems achieve the best results. Patients should ask about surgeon experience, case volumes, and availability of perioperative backup.
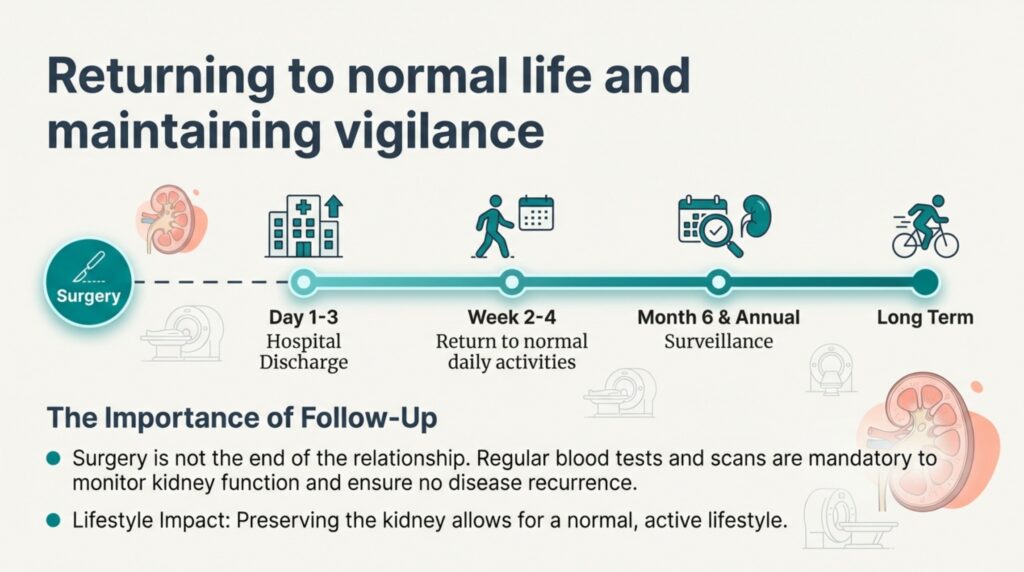
Postoperative course and follow-up
After RAPN:
Patients usually stay in hospital for 1–3 days.
A urinary catheter and sometimes a drain may be used temporarily.
Pain is generally less compared with open surgery.
Activity is gradually increased; heavy lifting is restricted for several weeks.
Follow-up includes wound checks, renal function tests, and imaging surveillance as per oncologic protocols (to detect recurrence and monitor kidney function).
Long-term follow-up is important; periodic imaging and kidney function monitoring are tailored to tumor pathology and patient factors.
Care for Patients from Bihar and Nearby Areas
Patients from Purnia, Katihar, Araria, Kishanganj, Saharsa, Supaul, other parts of Bihar, and neighbouring districts of West Bengal often travel for advanced kidney surgery.
Dr. Zaheen Khan, Urologist and Robotic Surgeon provides evaluation and robotic kidney surgery services for patients who are suitable candidates for kidney-saving procedures. Early diagnosis and timely treatment can protect kidney function and improve long-term quality of life.
Robotic Partial Nephrectomy is a modern, kidney-preserving surgery that offers effective cancer treatment with faster recovery and better long-term kidney health. When performed by an experienced urologist, it provides safe and reliable outcomes for many patients with kidney tumors.
If a kidney tumor is detected, early consultation with a urologist helps determine whether kidney-saving robotic surgery is possible.